






Socio demographic characteristics of the study participants
Between April and June 2016, a total total 465 patients with diabetes were recruited from three hospitals (~ 150/hospital) and 58% was female. The mean age of the participants was 49 years (SD:11) (Table 1) and female patients were younger than the male patients (mean age: 47 years; SD:11 vs. mean age:53 years SD:11; P < 0.001). More than 2/3rd of the patients (64.3%) completed primary education and the proportion was higher among males than females (72.6% vs. 58.2%; P < 0.001). Overall, 72.4% females were homemaker followed by 23.5% in service, 2.6% in business, 1.5% were day laborer and 1.1% unemployed. Overall, 31% males were involved in service followed by 29.9% unemployed, 28.4% in business and 10.7% were day laborer. The average household income ranged between 178.00 USD (IQR: 127, 255) and 637.00 USD (IQR: 407,891), and 1.5% households were living in extreme poverty. The age, level of education and occupation were significantly different between male and female patients (Table 1).
History of diabetes and pattern of diabetic care
About 3/4th of the study participants (75.7%) were first diagnosed as having diabetes by a doctor (MBBS) and other patients incidentally learnt about it when a laboratory test was performed for a different health concern. The mean age of the participants was 43 years (SD: 10.4) when they were first diagnosed as having diabetes and a female patient was diagnosed at a younger age (mean age (SD): 41 (10.0) years) than a male patient (46 (11) years; P < 0.001). The greater majority of the patients (95%) received treatment from a doctor when first diagnosed as having diabetes and 5% of the participants sought care from a provider other than a doctor, which included drug sellers in the pharmacy, traditional healers, village doctors, homeopathy practitioners, ayurvedic practitioner, health workers and paramedics.
Pattern of health care seeking
The majority of the patients (83.0%) sought health care within the past six months of the survey and 46% of them attended the study hospital OPD as their first choice for treatment. The remaining patients (54%) visited another facility before attending the study hospital OPD and among them 37.6% visited another tertiary hospital, 31.2% a private facility, 15.2% a diabetic clinic, 8.0% a government health facility and 8.0% a pharmacy. During the past visit 48.2% sought care for any issues related to diabetes and 51.8% sought care for a different health reason including infection (30.3%), muscle or bone problem (16.3%), heart problem (11.8%), abdominal problem (5.0%), eye related problems (4.7%), kidney problem (3.9%), respiratory problem (2.1%), neurological problem (2.1%), and women health issues (1.3%).
At the time of current visit, 40.9% of the patients attended the study hospital as their first choice of treatment and 59.1% visited another health facility before attending the study hospital. Those who visited another facility, 33.8% attended a government tertiary hospital, 6.2% attended a government primary or secondary hospital, 29.1% attended aprivate health facility, 24.4% BADAS and 6.5% attended a pharmacy (Table 2). Half of the patients visited the study hospital for seeking care for a health issue related to diabetes (50.1%), and 49.9% patients visited for a health issue not related to diabetes, such as, pain (26.3%), eye problem (23.6%) nonspecific complaints (21.9%), heart problem (7.9%), neurological problem (5.4%), kidney problems (4.0%), respiratory problems (4.0%), acute conditions (3.6%), and dental problem (3.2%).
Pattern of diabetic care
When the study participants were first diagnosed with diabetes, about 2/3rd of them (67.4%) started a diabetic care plan including drug, diet, and PA, followed by 6.4% on diet and drug, 9.0% on diet and PA, 4.9% on PA and drug, 7.5% on drug only, 0.2% on diet only, 0.6% were on PA only and 3.9% adopted no plan for diabetic care. At the time of survey, 60.1% of the patients reported to be on drug, diet and PA, 13.3% on diet and drug, 6.4% on diet and PA, 3.9% on PA and drug, 9.7% on drug only, 0.9% on diet only, and 1.3% on PA only and 4.5% adopted no plan for diabetic care (Table 2).
Overall, 86.9% patients reported to have taken an anti-diabetic drug (either insulin /or a tablet) and 66.9% patients have reported to have an associated comorbidity for which they have been taking treatment including hypertension (71.1%), eye complications (43.7%), heart disease (26%), neuropathy (11.9%), and chronic kidney disease (7.7%). One third of the patients (33.2%) reported discontinuaction of anti-diabetic drug (or reduced the dose) over the past six months without consulting a doctor irrespective of having an associated co morbidity or not (Table 2).
Behavioral risks among diabetic patients
Two thirds of the patients (67.7%) had two or more behavioral risk factors. Overall, 87.5% patients reported regular vegetable consumption and 19.8% patients reported regular fruits consumption. Half of the patients (50.3%) reported regular consumption of extra salt with meal and 32.7% had reported consumption of any form of tobacco (either chewing or smoking). The average IPAQ MET-score was 2014.7 (SD: 3137.5). Physical activity was low in 27.1%, moderate in 54.4% and high in 18.5% patients (Table 3).
Cardiometabolic risks among diabetic patients
The greater majority of the patients (98%) had hyperlipidemia, 46% were overweight and 24.7% were obese, and 34.2% had raised systolic or diastolic blood pressure. Among those who had hyperlipidemia, Overall, 97.6% had low HDL, 69.7% had raised triglycerides, 35.1% had a raised LDL level, and 9.2% had a raised total cholesterol level beyond the normal range (Table 3). The total cholesterol level was significantly correlated with LDL (corr: 0.86, P < 0.001), triglycerides (corr: 0.46, P < 0.001) and HDL (corr: 0.16, P = 0.001).
Glycemic control with diabetic care pattern, behavioural risks, cardiometabolic risks
One third of the patients (31.4%) had glycemic control (HbA1C: < 7.0%) and the level of HbA1C increased by 11.5% with increase of duration of diabetes by one year (corr: 0.115, P = 0.013). However, there was no difference in glycaemia control across age, sex, education and socio demographic status of the study patients(Supplementary Material).
Glycemic Control and Diabetic care
Glycemic control was better among those who maintained diabetic care plan of diet and PA without any drugs than those who had followed any other diabetic care plans (OR: 0.33, 95% CI 0.15–0.68). The odds of uncontrolled diabetes were more than two times higher if duration of diabetes was more than 5 years (OR: 2.66, 95% CI 1.78–4.00), two times higher if a patient was treated by drug only (OR:2.26, 95% CI: 1.02-4.99) and 87% higher if a patient visited the study hospital OPD for diabetic care (OR: 1.88, 95% CI 1.23–2.74), more than otherwise. . However, the type of provider, seeking medical care in the past six months, and the type of facility where diabetic care was sought when diabetes was first diagnosed were not associated with uncontrolled diabetes (Fig. 1 and Supplementary Material).
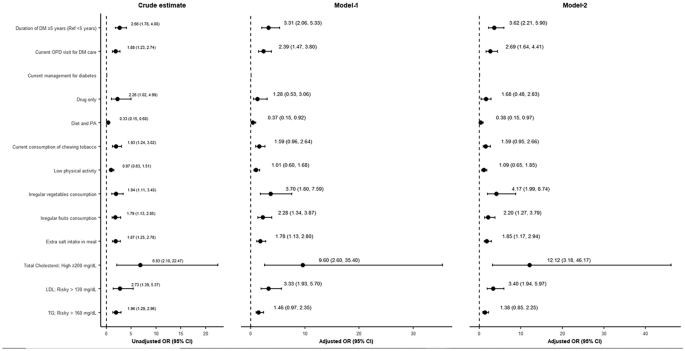
Factors attributed to poor glycemic control among ambulatory diabetic patients in tertiary care settings. (Multivariable logistics regression model for adjusted odds ratio). Note: Model 1 was adjusted for diabetes care, behavioral risk factors, and metabolic risk factors; Model 2 was adjusted for DM care, behavioral risk, and metabolic risk, age, sex, education and occupation. The result was statistically significant based on 95%, with level of significance at P < 0.05 for adjusted models and 90% with level of significance at P < 0.1 for unadjusted variables. Abbreviations: PA= Physical activity.
Glycemic Control and Behavioral risks
The odds of uncontrolled diabetes was 93% higher if a patient had consumed chewing tobacco than otherwise (OR:1.93, 95% CI 1.24–3.02), 94% higher in those who had irregular vegetable consumption than those who had regular vegetable consumption (OR: 1.94, 95% CI 1.11–3.40), 79% higher in those who had irregular consumption of fruits (OR: 1.79, 95% CI 1.13–2.85), and 87% higher if a patient had consumed extra salt in meal in a day (OR:1.87, 95% CI 1.20–2.91). However, smoking tobacco and physical activity were not associated with uncontrolled diabetes (Table 2 and Supplementary Material).
Glycemic control and Cardiometabolic risks
The odds of uncontrolled diabetes was more than six times higher in those who had total cholesterol beyond the normal range (OR:6.4, 95% CI 1.60–25.62), more than two times higher in those who had LDL beyond the normal range (OR:2.73, 95% CI 1.39–5.37) and 96% higher in those who had triglyceride level beyond the normal range (OR: 1.96 95% CI1.29–2.96) than otherwise. However, there was no association of uncontrolled diabetes with BMI, raised blood pressure and having an associated comorbidity (Fig. 1 and Supplementary Material).
Factors attributed to uncontrolled diabetes
Figure 1 (Model 1) demonstrated that the odds of uncontrolled diabetes was three times higher in those who had diabetes for more than 5 years compared to those who had diabetes for less than 5 years (OR: 3.31, 95% CI 2.04–5.27), and two times higher for those who visited the hospital OPDs for seeking care for diabetes compared to those who visited the hospital OPDs for other health reasons (OR: 2.39, 95% CI 1.47–3.80). For the behavioral risks, the odds of uncontrolled diabetes was there times higher in those who had irregular vegetable consumption than those who had regular consumption (OR: 3.70., 95% CI 1.80–7.59), two times higher in those who had irregular consumptions of fruits than those who had regular consumption (OR: 2.28, 95% CI 1.34–3.87), and 78% higher risk in those who consumed extra salt in any meal a day than those who did not (OR: 1.78, 95% CI 1.13–2.80). For the metabolic risks, the odds of uncontrolled debates was nine times higher in those who had raised total Cholesterol level compared to those who did not (OR: 9.6, 95% CI 2.60–35.4) and three times higher in those who had a raised a LDL level compared to those who did not (OR: 3.33, 95% CI: 1.93-5.70). After adjusting for age, sex, education and occupation( model 2), the association of these factors with uncontrolled diabetes remained unaltered and the association of total cholesterol with uncontrolled diabetes became stronger (OR:12.12, 95% CI: 3.18-46.17). Consumption of chewing tobacco, low physical activity and TG level were not found associated with uncontrolled diabetes in any model(Fig. 1).
link
More Stories
UniHealth Hospitals Limited Announces the Commissioning of its Advanced Tertiary Care, Multi-Specialty Hospital in Navi Mumbai
Predictors of opportunistic infections among people living with HIV: a prospective cohort study from a tertiary care setting in India
The impact of DRG payment reform on inpatient costs for different surgery types: an empirical analysis based on Chinese tertiary hospitals